
Evidence-Based Sensory Intervention Explained for Parents
Unlock the benefits of evidence-based sensory intervention explained. Discover how scientifically-backed strategies can support your child's daily activities.
Evidence-Based Sensory Intervention Explained for Parents
TL;DR:
- Evidence-based sensory interventions use scientifically validated strategies to help children manage sensory input and participate in daily activities effectively. Ayres Sensory Integration (ASI) is a structured, therapist-led approach with strong evidence, while passive techniques and caregiver training also show significant benefits for regulation and participation. Proper implementation requires individualized assessments, caregiver involvement, and embedding strategies into routines for meaningful, sustainable progress.
Evidence-based sensory intervention is defined as the use of scientifically validated strategies to help children manage sensory input and improve their participation in daily activities. The formal clinical term is sensory-based intervention, or SBI, and it sits within the broader field of occupational therapy. Ayres Sensory Integration (ASI) and deep pressure tactile methods are the two most rigorously studied approaches in this category. As a parent or educator, understanding what separates a clinically sound sensory intervention from a well-meaning but unsupported activity is the first step toward getting a child the right support.
What are the main types of evidence-based sensory interventions?
Sensory-based interventions span a wide range of techniques, and not all carry the same level of evidence. The four main categories are ASI therapy, passive sensory techniques, caregiver training, and environmental modifications.

Ayres Sensory Integration is child-directed, play-based, and delivered by a postgraduate-trained occupational therapist. A 2026 systematic review on ASI evaluated 9 RCTs with 344 participants and found strong evidence that ASI helps autistic children meet individualized occupational goals. That means children showed measurable gains in the specific daily tasks that mattered most to their families, such as dressing independently or tolerating a school cafeteria.
Passive sensory techniques include weighted blankets, firm massage, and deep pressure input. A 2025 systematic review covering 21 studies found strong evidence that deep pressure tactile input improves sleep and regulation. These techniques are adult-led and typically used to calm or prepare a child’s nervous system before a demanding activity.
Caregiver training is one of the most underrated categories. Strong evidence from 5 studies shows that parent and teacher training in sensory strategies leads to improved functional performance at home and school. When caregivers understand why a child seeks or avoids certain sensory input, they respond more effectively and consistently.
Environmental modifications round out the toolkit. Sound-absorbing materials, calm color palettes, and designated refuge spaces are evidence-based classroom adaptations that reduce sensory overload before it starts.
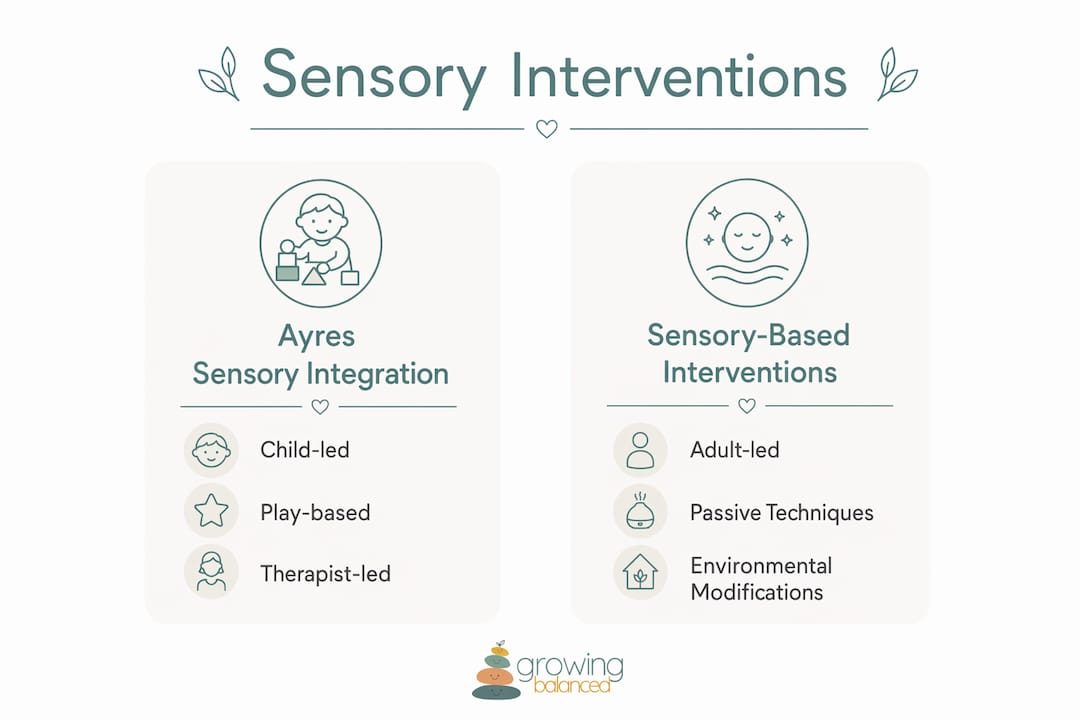
| Feature | Ayres Sensory Integration (ASI) | Sensory-Based Interventions (SBIs) |
|---|---|---|
| Who leads it | Trained OT therapist | Parent, teacher, or caregiver |
| Structure | Child-directed, play-based | Adult-directed, passive |
| Setting | Clinical or school OT room | Home, classroom, community |
| Evidence strength | Strong (5 RCTs for OT goals) | Strong for specific inputs (deep pressure) |
| Primary goal | Occupational participation | Regulation and sensory tolerance |
Pro Tip: Ask your child’s occupational therapist whether they have completed specific ASI training and whether they use fidelity measures. This tells you whether the therapy your child receives is true ASI or a sensory-informed approach, which are both valid but serve different purposes.
What does the latest research say about effectiveness?
The evidence base for sensory interventions has grown considerably, but it comes with important nuances. 98% of pediatric occupational therapists working with autistic children report using sensory-based strategies clinically. That near-universal adoption reflects genuine clinical utility, but it also means the quality of implementation varies widely.
ASI shows strong evidence for improving individualized occupational goals, but the same 2026 review found only moderate evidence for reducing behaviors like irritability or non-compliance. This distinction matters. If a family’s primary goal is for their child to participate in morning routines, ASI is well-supported. If the goal is to eliminate meltdowns entirely, the evidence is less clear, and a broader behavioral or co-regulation approach may be needed alongside sensory work.
“Sensory tools like weighted vests provide only immediate regulation and must be part of a larger coordinated approach embedding strategies into routines.” — Royal College of Occupational Therapists, March 2026
The RCOT guidance also recommends that sensory interventions be time-limited and discontinued if no measurable progress is observed within a set timeframe. This protects children from prolonged programs that are not working and redirects resources toward approaches that do.
Pro Tip: When reviewing your child’s sensory program, ask for measurable participation outcomes, not just behavioral observations. “He seems calmer” is not the same as “he now completes morning dressing independently four out of five days.”
How do sensory interventions differ from related therapies?
Confusion between ASI, sensory diets, and unstructured sensory activities is one of the most common pitfalls in sensory support. Conflating SBIs with ASI therapy leads to ineffective programs that lack a clear therapeutic rationale. Here is how to tell them apart:
- ASI therapy requires a postgraduate-trained therapist, a fully equipped sensory gym, and adherence to a fidelity checklist. It is structured, individualized, and goal-directed.
- Sensory-based interventions are adult-led strategies like providing a weighted lap pad before a writing task or offering a chewy snack before a transition. They are valid tools but not a substitute for ASI.
- Sensory diets are scheduled sequences of sensory activities designed to maintain a child’s optimal arousal level throughout the day. They require clinical reasoning to design and should not be generic templates copied from the internet.
- Unstructured sensory play (a bin of kinetic sand, a trampoline in the backyard) has developmental value but is not a clinical intervention.
Frameworks like Dunn’s Sensory Processing Model and the Pyramid of Learning help occupational therapists identify whether a child’s behavior reflects a sensory threshold issue, a postural stability need, or an emotional regulation challenge. Clinical reasoning focused on sensory threshold patterns produces targeted interventions rather than generic tool selections. A fidget spinner handed to every child in a classroom is not sensory intervention. A fidget tool selected because a specific child has a high sensory threshold for proprioceptive input, confirmed through a sensory profile assessment, is.
The distinction between ASI and SBIs is not about which is better. It is about matching the right level of intervention to the child’s assessed needs.
How can parents and educators apply these interventions daily?
Practical implementation starts with individualized assessment, not tool shopping. Work with a qualified occupational therapist to complete a formal sensory profile before selecting any strategies. The sensory tools in classrooms guide from Growingbalanced explains why embedding strategies into routines outperforms reactive tool use every time.
Follow these steps to build a sound sensory support plan:
- Complete a sensory profile assessment with an OT to identify the child’s specific sensory thresholds and patterns across all eight sensory systems.
- Select strategies proactively. Proactive use before sensory crises produces better outcomes than reaching for a tool after a meltdown has already started.
- Embed strategies into existing routines. A two-minute deep pressure activity before homework, or noise-canceling headphones during transitions, works because it is predictable and consistent.
- Train all caregivers. Teachers, teaching assistants, and parents need to understand the rationale behind each strategy. Inconsistent application reduces effectiveness significantly.
- Adapt the environment. Review the types of sensory accommodations available for classrooms, including lighting adjustments, seating options, and designated calm spaces.
- Monitor with measurable goals. Track participation outcomes, not just behavior. Set a review date and adjust the plan if progress stalls.
Pro Tip: Build sensory strategies into visual schedules so children know what to expect. Predictability reduces anxiety, which in turn reduces the sensory load the child’s nervous system has to manage.
What I’ve learned about sensory interventions after years in this field
The gap between how popular sensory tools are and how well they are used in practice is striking. Weighted blankets and sensory bins appear in nearly every classroom and many homes, yet the clinical reasoning behind their use is often absent. A tool without a rationale is just an object.
What the research consistently shows, and what I have seen play out in practice, is that caregiver engagement is the single biggest predictor of success. A child who receives excellent OT sessions twice a week but returns to an environment where no one understands or applies the strategies will make slower progress than a child whose parents and teachers are trained and consistent.
The other point worth making directly: sensory interventions are not a permanent fix. The RCOT’s 2026 guidance is clear that programs should be time-limited and goal-directed. If a strategy has been in place for three months with no measurable change in participation, it is time to reassess. Holding onto an ineffective program because it feels supportive is not the same as providing effective support.
The future of this field lies in better clinical reasoning tools and stronger caregiver coaching models. Growingbalanced’s approach, combining visual routines with OT-informed sensory resources, reflects exactly the kind of integrated, everyday support the evidence points toward.
— Kelsey
How Growingbalanced supports your sensory intervention journey
Growingbalanced is built for exactly the situation most parents and educators face: you understand that your child needs sensory support, but translating clinical recommendations into daily life is harder than it sounds. The platform’s visual schedules and daily routines make it straightforward to embed sensory strategies into predictable sequences that children can follow independently. Growingbalanced also offers sensory profiles, co-regulation scripts, and a resource library of OT-informed printables designed for both home and classroom use. Whether you are just starting to explore sensory support or refining an existing plan, the tools at Growingbalanced give you a structured, evidence-informed starting point without needing a clinical background to use them.
FAQ
What is a sensory-based intervention?
A sensory-based intervention is an adult-led strategy that uses specific sensory inputs, such as deep pressure, weighted tools, or movement, to help a child regulate their nervous system and participate in daily activities. It differs from Ayres Sensory Integration, which is a structured, therapist-led clinical therapy.
What does the evidence say about deep pressure techniques?
A 2025 systematic review of 21 studies found strong evidence that deep pressure tactile input, including weighted blankets and firm massage, improves sleep and regulation in children with sensory processing differences.
How is ASI different from a sensory diet?
ASI is a postgraduate-trained therapist-led therapy delivered in a clinical setting with fidelity checks. A sensory diet is a scheduled sequence of sensory activities designed by an OT for use at home or school, and it is a sensory-based intervention, not ASI therapy.
When should a sensory program be reconsidered?
The Royal College of Occupational Therapists recommends discontinuing a sensory program if no measurable progress in functional participation is observed within a set timeframe. Ongoing programs without clear goals and review dates are not considered best practice.
Can teachers implement sensory interventions without an OT?
Teachers can apply OT-recommended sensory strategies, such as environmental modifications and scheduled movement breaks, but the initial assessment and program design should always involve a qualified occupational therapist to match strategies to the child’s specific sensory profile.
Recommended
- Ayres Sensory Integration Explained for Parents · Growing Balanced Blog
- Sensory Seeking Behavior Explained for Parents · Growing Balanced Blog
- Home program components: OT recommendations for sensory kids · Growing Balanced Blog
- Sensory Tools in Classrooms: What Educators Need to Know · Growing Balanced Blog